Уреаплазма - типичный представитель транзиторной микрофлоры
- (условно-патогенная микрофлора мочеполовых органов, постоянное присутствие
которой нехарактерно для здорового человека и которая при определенных условиях
может вызывать воспалительный процесс в мочеполовых органах и передаваться
половым путем). Поэтому уреаплазму нужно рассматривать как инфекцию.
Способы заражения уреаплазмой.
Заражение урогенитальными — то есть поражающими
мочеполовой тракт — уреаплазмами происходит половым путем, возможна также
передача инфекции от матери к ребенку внутриутробно и во время родов.
Симптомы уреаплазмы.
Клиническая картина уреаплазменной инфекции практически
отсутствует. У 95% женщин заболевание протекает бессимптомно. Если уреаплазма
проявляется, то больная жалуется на выделения из влагалища, частое, болезненное
мочеиспускание, боли в низу живота. У мужчин первый период инфицирования
уреаплазмой (от нескольких дней до одного месяца) чаще проходит также бессимптомно,
по истечении скрытого периода наиболее частым проявлением становится негонококковый
уретрит, характеризующийся следующими симптомами: жжением и зудом в области
мочеиспускательного канала, резью при мочеиспускании, небольшими слизистыми
выделениями, выходное отверстие из мочеиспускательного канала склеивается гноем,
сама моча мутнеет.
Чем опасна уреаплазма.
У мужчин уреаплазма преимущественно заселяет уретру и
крайнюю плоть. При отсутствии лечения процесс продолжает распространяться на
простату, ткань яичек (развивается орхоэпидимит), семенные пузырьки. У женщин
уреаплазма колонизирует влагалище, реже шейку матки и уретру; возбудитель
вызывает уретриты, цервициты и воспалительные поражения тазовых органов
(сальпингиты, оофориты, эндометриты, аднекситы и др.).
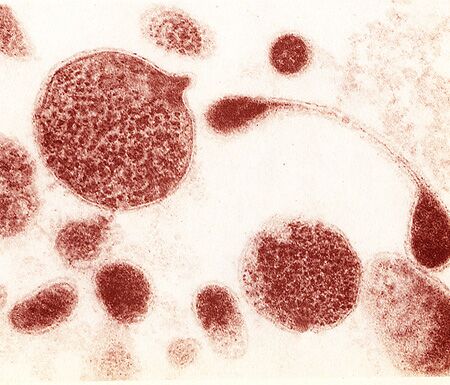
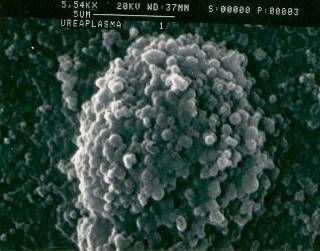
электронная микроскопия уреаплазмы. Картинки с сайта:
http://www.ureaplasma.info
Уреаплазма и беременность.
Уреаплазма может стать причиной самопроизвольного
прерывания беременности на ранней стадии и даже привести к бесплодию.
Уреаплазма при беременности опасна еще и тем, что во время родов ребенок
может заразиться, проходя по инфицированным родовым путям матери. Лечение
во время беременности может отрицательно сказаться на развитии ребенка.
Вот почему так важно диагностировать заболевание и провести грамотное
лечение еще до наступления беременности.
Диагностика уреаплазмы.
В настоящее время чаще всего используютс
я следующие методы – ПЦР (полимеразная цепная реакция), выявление в
крови специфических антител и культуральные метод (высевание микробов
и их выращивание на искусственной питательной среде).
Лечение уреаплазмы.
Лечение уреаплазменной инфекции проводится в течение
10-14 дней назначенными врачом антибиотиками. Конкретная схема лечения
уреаплазмы может определяться только врачом, владеющим всей информацией
о пациенте (осмотр, анамнез, анализы).
Classification
информация взята с сайта www.ureaplasma.info
Taxonomy:
Kingdom Bacteria;
Phylum Firmicute(Tenericutes)s;
Class Mollicutes;
Order Mycoplasmatales;
Family Mycoplasmataceae;
Genus Ureaplasma;
Ureaplasma urealyticum
Геном Ureaplasma urealyticum секвенировали, потому что она болезнетворная, опасная бактерия, которая всем жить мешает. Но может быть из чисто научного интереса или потому что последнее время всех пытаются секвенировать, для того чтобы найти там что нибудь интересное, а возможно и полезное.
Description and Significance
Ureaplasma urealyticum is a bacterium that is found in the urogenital tracts of humans. It stains gram negative, but that is because it lacks a cell wall. This organism can exist as normal commensal flora in the reproductive tract (especially in women) and remain undetected unless specifically tested for. Women with this infection often experience fertility problems and can even be rendered infertile. Infected mothers can also transmit the infection to their baby. Often the babies are born prematurely and are prone to diseases like pneumonia and meningitis. It can also affect the babies’ respiratory tract. U. urealyticum is also found in males, but is less common. People infected with U. urealyticum can be treated with an assortment of medications. U. urealyticum has one of the smallest sequenced genomes. It is often associated with the Mycoplasmas, a group which includes human mucosal pathogens. Unique to this genus is the ability to generate ATP mostly by the hydrolysis of urea. Current research includes determining how many people carry the infection and finding out more specifically the conditions that it lives in as well as its effect on infants and if its presence is correlated with other diseases.
Genome
U. urealyticum has a double-stranded DNA circular chromosome of 751,719 bp. This genome is unique because it is smaller than any other sequenced microbial genome, except for M. genitalium, a closely related human mucosal pathogen. As has been observed with othe r Mollicutes, its genome appears to have undergone significant reduction. It also has a relatively low G+C content (25.5%), making it more A+T rich than any other microbial genome that has been sequenced so far. It contains 613 protein-coding genes and 39 genes that code for RNAs (rRNAs, tRNAs, ribonuclease P rnpB and a tmRNA) . Overall, these genes make up 93% of the U. urealyticum genome. Of the protein-coding genes, researchers have found that 53% of those genes have specific biological roles. The genome lacks pseudogenes. It has a total of 605 ORFs, 313 of which have been identified as functional and 292 are hypothetical.
U. urealyticum has six closely related iron transporters. They appear to have arisen by gene duplication. Researchers believe that U. urealyticum increased its number of iron transporter genes in order to increase its capacity to import more iron. Although U. urealyticum is similar to the Mycoplasmas, its evolutionary divergence is evident from analysis of gene order. There are 76 proteins coded for by U. urealyticum that have a function and/or cellular location that is not found in two different mycoplasma genomes (M. genitalium and M. pneumoniae). Most of these genes are involved in ATP production via urea hydrolysis (something unique to ureaplasmas) and in iron acquisition. It is speculated that the phenotype of U. urealyticum is the result of its unique set of genes for energy production and respiration. U. urealyticum produces a major surface antigen (gene MBA) that is believed to help the organism evade the host’s immune system. MBA has at least 5 other paralogs dispersed throughout the genome. This gene product defines the 14 different U. urealyticum serovars. None of the type I restriction/modification genes are complete in U. urealyticum, and they are disrupted by indel events (ref is Glass paper). Another unique characteristic of the genome is that it lacks GroEL and GroES heat shock proteins/chaperonins. More surprising is that U. urealyticum lacks the protein FtsZ, a cell-division protein. All bacterial genomes to date, except for chlamydias and Aeropyrum pernix, have FtsZ. It is thought that FtsZ is an essential part of the cell-division mechanism.
The entire genome was sequenced in 2000 at the University of Alabama- Birmingham and has an accession number of AF222894.
Cell Structure and Metabolism
Ureaplasma urealyticum are some of the smallest known organisms that can self-replicate on laboratory media. U. urealyticum is often associated with Mycoplasmas and shares a similar cell structure. Mollicutes and Ureaplasma urealyticum, are known for having the following characteristics: (1) They range from 125-250 nm in size. (2) They are highly pleomorphic, because they lack a cell wall. (3) They are bound by a triple-layered “unit membrane” that contains a sterol, causing them to stain as gram negative. (4) Ureaplasma urealyticum can reproduce in cell-free media, agar. (The center of the colony is usually embedded beneath the surface.) However, they require the addition of cholesterol, which is required to make their “unit membrane.” (5) Mycoplasmas (and therefore also U. urealyticum) are completely resistant to penicillin because they lack a cell wall, but are inhibited by tetracycline or erythromycin. (6) Growth o f Mycoplasmas is inhibited by specific antibodies. (7) Mollicutes generally lack TCA cycle (8) Mycoplasmas have an affinity for mammalian cell membranes.
Ecology
U. urealyticum is found in the genitourinary tract of humans and grows in a pH range of 5-9. .U. urealyticum are often found accompanied with other species, such as M. hominis. Three species have been isolated together from the surface of the genitourinary tract mucosa: Mycoplasma hominis, Ureaplasma urealyticum, Mycoplasma genitalium. There is some dispute as to U. urealyticum’s relation to its host. Most researchers agree that U. urealyticum is part of the normal vaginal flora and lives as a commensal organism doing little or no harm to the host. U. urealyticum was isolated from the cervix and vagina from 52-76% post pubertal girls in the absence of symptoms suggesting that the organism is commensal. It becomes pathogenic when it takes advantage of the host’s supplies. In women, Ureaplasma urealyticum is most commonly found in the vagina, upper and lower genital tract. Normal-term babies born from Ureaplasma urealyticum positive mothers sometimes have the organism colonize skin and mucosal sites; and pre-term infants have a much higher colonization. In addition, U. urealyticum and M. hominis have been found together in the blood stream of women with postpartum fever and infection. U. urealyticum can also be isolated from amniotic fluid. Its adverse effects on pregnancy occur mostly when the organism travels up the upper reproductive tract. This can lead to a chronic infection in some patients, and continual isolates can be taken from the endometrium in these cases. Ureaplasma urealyticum is less commonly found in men. There is a study that shows that U. urealyticum can be found co-existing with N. gonorrhoeae in the male urethra; it was also isolated on its own from the male urethra and genital tract.
Pathology
Ureaplasma urealyticum can be transmitted in various ways, including directly by sexual transmission through direct contact between couples, vertically from mother to offspring, or through hospital-acquired infections from transplanted tissues. Until a female is specifically tested for an infection, this microorganism can live as normal flora in her reproductive tract and remain undetected. Thus, the symptoms for this bacterium can vary from person to person. Some of the most common symptoms for women associated with this bacterium include infertility, recurrent pregnancy loss, pelvic pain, premenstrual symptoms like spotting between menstrual cycles, and vaginal symptoms like uterine infection. Other general symptoms associated with this bacterium include a chronic sore throat, gall stones, kidney stones, red itchy eyes, chronic fatigue, blindness and pain upon looking at light, headaches and frequent passing out, lack of mind coordination, arthritis, asthma, heart attacks, strokes, cerebral palsy, high blood pressure, nasal polyps, stuffy nose in newborns, coughing, belly or muscle pain, burning in the stomach, bloody diarrhea, and anal itching and bleeding. The infections associated with Ureaplasma urealyticum can be contagious, and if an infected person coughs in one’s face or if one accidentally touches the infected person’s nasal or eye secretions, the recipient becomes infected. If one is treated for their infections when they have the local symptoms mentioned above, they can be easily cured. However, if undetected and untreated, the infection can spread to other parts of the body and potentially cause damage to the nervous system, muscular system, or the joints. The bacterial infections that are caused by Ureaplasma urealyticum can also lead to fertility problems such as tubal disease, recurrent miscarriages, decreased sperm motility, and poor post coital tests. Furthermore, Ureaplasma urealyticum has been attributed to many diseases in the lower urogenital tracts of humans. Other diseases that are caused by this microorganism include chorioamnionitis, an infection of the amniotic membrane and the amniotic fluid. Stillbirth can also be caused by U. urealyticum. It is also associated with non-gonococcal urethritis, an infection in the urethra that is not caused by gonorrhea . Additionally, this bacterium can attack the cerebrospinal fluid and cause pleocytosis, which is an increase in cell count. Ureaplasma urealyticum is also noted to often cause infectious arthritis in people who have hypogammaglobulinemia, a deficiency in immunoglobulin.
Research shows that the presence of this microorganism in human in vitro semen or in female genital tracts can result in a decline in the pregnancy rate per embryo transfer. This microorganism is becoming a very important opportunistic pathogen in pregnant women. The placental infections in pregnant women mentioned earlier can lead to the birth of premature babies. These premature infants often become prone to diseases such as septicemia (the presence of bacteria in the blood), pneumonia, and meningitis (inflammation of the membranes in the brain). Low birth weight infants can later face death if they acquire a Ureaplasma urealyticum infection in their lower respiratory tract. Although many risk factors have been identified regarding the colonization of this microbe in the lower genitourinary tract, more information is needed to identify the risk factors concerning host immune response to infection by Ureaplasma urealyticum.
Treatments
According to a study done at the University of Kurtkukale Faculty of Medicine (Kurtkkale, Turkey) Ureaplasma urealyticum showed no resistance to doxycycline, 4.2% resistance to tetracycline, 12.5% resistance to erythromycin and 16.7% resistance to ofloxacine. As a result, physicians prescribe 100mg of doxycycline twice a day. Other physicians have also found 500 mg of azithromycin twice a week to be effective. These treatments are usually long-term. Other research on using fluoroquinolones and/or clindamycin for treatment is still underway.
Current Research
According to a study published in the January 2008 issue of the American Journal of Obstetrics & Gynecology, researchers from the University of Alabama--Birmingham Medical School and the Drexel University College of Medicine determined that 23% of neonates born between a 23 and 32 week gestation period had umbilical blood cultures for Ureaplasma urealyticum and Mycoplasma hominis. This study is looking into the possibility that antibiotic treatment of women likely to deliver an early gestational age infant might reduce subsequent neonatal morbidity and mortality. Another study focused on determining if Ureaplasma urealyticum can elicit an inflammatory response. White blood counts were determined for more than 50 premature infants. Fifteen tested positive for U. urealyticum. The increased WBC counts after birth suggested that U. urealyticum is a pathogen capable of eliciting an inflammatory response. Anothe r study focused on finding if the colonization of Ureaplasma Urealyticum had any correlation to the presence and development of funisitis, or inflammation of the umbilical cord. They found a correlation between funisitis and the presence of U. urealyticum. This is the first study to suggest this correlation. The study also recommends that antibiotics be used to prevent funisitis, since it is one of the causes of preterm labor. информация взята с сайта:
http://microbewiki.kenyon.edu